Without contrast "Acute Stroke MRI Protocol"
Role of Diffusion:
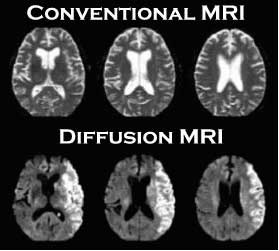
Most sensitive and relatively specific.
Based on principle of restriction of normal Brownian motion of water molecules in infarcted tissue.
Infarct seen as an abnormal white area and described as an area of restricted diffusion.
Role of FLAIR:
Sensitivity to pick an infarct is arbitrarily comparable to CT.
If an infarct seen on diffusion and not seen FLAIR called FLAIR / Diffusion Mismatch indicate hyper acute infarct - reversible ischemic changes and salvageable tissue or tissue at risk.
If changes are marked on FLAIR indicate already infracted and non salvageable tissue.
Role of T2* GRE:
Used to demonstrate hemorrhage or hemorrhagic transformation in the region of infarct as an alternative to CT.
Area of bleed appear dark due to paramagenetic effect of blood degradation products.
MR Angiography of brain and neck:
To demonstrate any major vessel stenosis or occlusion.
No contrast required.Accuracy acceptable.

 ADC
ADC
READ MORE CLICK THE FOLLOWING LINKS:
- 3-Plane loc
- Axial Diffusion
- Axial EPI GRE
- Axial EPI Flair T2
- Axial 2D TOF (coarse 10mm slices, corpus callosum to arch)
- 3D TOF MRA if there is no perfusion
If required you can add the following sequences according to the Lesion
- Coronal T2 for periventricular/basal ganglia infarct
- T1 Axial for the acute bleed-hemorrhage or hemorrhagic transformation in the region of infarct
Optional Sequences in "Acute Stroke MRI Protocol"
- Ax Permeability (30 sec delay)
- Cor CEMRA: Carotids/Arch (22g insyte: 10cc Gadovist @ 1.5cc/sec. 30cc saline @ 1.5cc/sec, cover vertebral and carotid arteries posterior to anterior, aortic arch to top of COW)
- Axial Perfusion (0 Delay)
- Axial T1 Post-Contrast
Role of Diffusion:
Most sensitive and relatively specific.
Based on principle of restriction of normal Brownian motion of water molecules in infarcted tissue.
Infarct seen as an abnormal white area and described as an area of restricted diffusion.
Role of FLAIR:
Sensitivity to pick an infarct is arbitrarily comparable to CT.
If an infarct seen on diffusion and not seen FLAIR called FLAIR / Diffusion Mismatch indicate hyper acute infarct - reversible ischemic changes and salvageable tissue or tissue at risk.
If changes are marked on FLAIR indicate already infracted and non salvageable tissue.
Role of T2* GRE:
Used to demonstrate hemorrhage or hemorrhagic transformation in the region of infarct as an alternative to CT.
Area of bleed appear dark due to paramagenetic effect of blood degradation products.
MR Angiography of brain and neck:
To demonstrate any major vessel stenosis or occlusion.
No contrast required.Accuracy acceptable.
ADCREAD MORE CLICK THE FOLLOWING LINKS:









No comments:
Post a Comment