The sternum and sternoclavicular joints are difficult to evaluate with plain radiographs. The value of CT in assessing lesions of the sternum and sternoclavicular joints has been well documented, but the potential role of MRI has not been emphasized. We present the MRI techniques, normal appearances and a spectrum of abnormalities, and emphasize the role of MRI as a useful radiological investigation for the sternum and sternoclavicular joints.
MRI SERNOCLVICULAR JOINT PROTOCOL
Axial T1
Axial T2 Fat Sat
Coronal T1
Coronal STIR
Sagittal T2 Fat Sat
PD Fat Sat Axial
Technique
Breath-hold images were obtained in threeorthogonal planes, coronal, sagittal and axial,using a general purpose body array coil on a1.5 T Siemens Vision scanner (Siemens, Erlangen,Germany). Coronal images were obtained in two oblique planes, one parallel to the manubrium and the other parallel to the body of the sternum.
Both T1 and T2 weighted images were acquired. Short tau inversion recovery (STIR) or fat suppressed T2 weighted images were acquired in the optimal plane to depict the pathology. Respiratory gating was required for STIR sequences only
The sternum is optimally demonstrated in the sagittal plane with clear delineation of the manubrium, the body of the sternum and the xiphoid process. The outer cortex and central marrow are well seen . Coronal images are obtained in two planes for clear views of the manubrium and body of the sternum as they are angulated at the manubriosternal junction. The axial images provide additional information, particularly in the evaluation of congenital chest wall deformities.
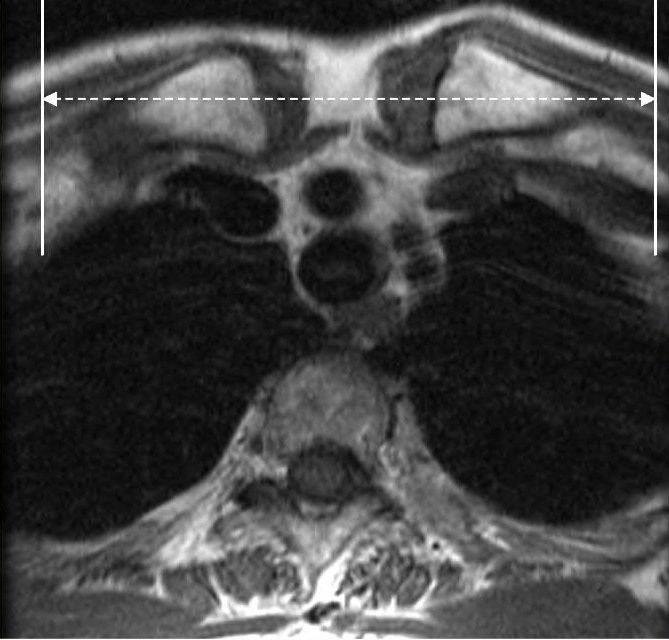
Magnetic resonance (MR) imaging is of great value as a secondary modality. It can help clarify CT findings and can provide additional information about the bone marrow and soft tissues adjacent to the sternum . At MR imaging, the sternal anatomy is best depicted with T1-weighted spin-echo pulse sequences. The coronal plane displays the articular surfaces, as well as the intraarticular disk; the sagittal plane is useful for depicting the costoclavicular ligament; and the axial plane best delineates the anterior and posterior parts of the sternoclavicular joint capsule and the anterior and posterior sternoclavicular ligaments . Normal findings that should not be mistaken for disease include small amounts of joint fluid, nonfatty bone marrow, and poorly defined cortical margins
Axial Plane: Center on Sternum on coronal scout and prescribe plane perpendicular to line through sternum. Scan through SC joint.
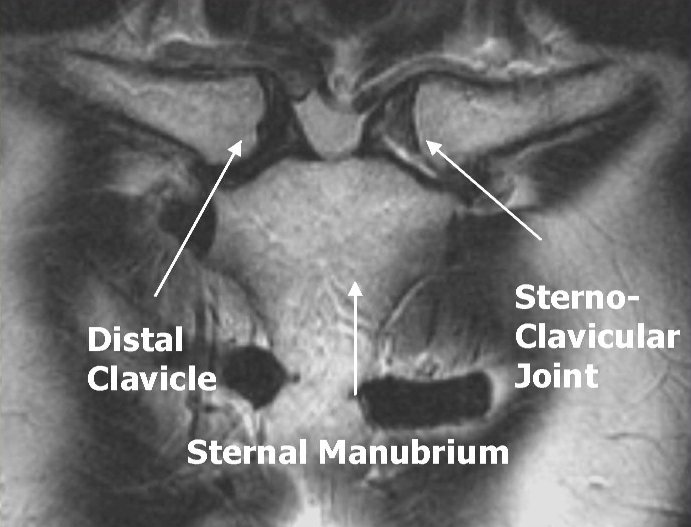

Coronal Plane: Prescribe perpendicular to SC join. Scan through both clavicle heads


Sagittal Plane: Prescribe plane with line that touches the anterior cortex of the sternum and clavicle heads. Scan through both SC joints.

The sternoclavicular articulation is a double arthrodial joint. The parts entering into its formation are the sternal end of the clavicle, the upper and lateral part of the manubrium sterni, and the cartilage of the first rib. The articular surface of the clavicle is much larger than that of the sternum, and is invested with a layer of cartilage, which is considerably thicker than that on the latter bone. |









